
Electric Stim Pad Placements
Updated May 23, 2026
This page pairs with Electric Stimulation Programs.
Electric stimulation for increasing muscle strength, circulation and decreasing pain is something I very much believe in. However, EMS for me is currently on the back burner, with this page supporting my older physical therapy-related blogs on electric stimulation.
I'm hoping to work this in with SpineFITyoga, as I think electric stimulation (EMS especially and less so TENS) has tremendous potential to help people with more severe neck and back pain. It can rapidly and substantially decrease pain while at the same time increasing spine stabilization strength so that you can better perform the rest of SpineFITyoga.
However, I would rather not push electric stim that hard because SpineFITyoga is awesome as is. Still, it's the truth that electrical stimulation, DONE PROPERLY, can absolutely accelerate progress, perhaps being particularly effective, especially for those with fibromyalgia, central sensitization, or chronic widespread pain-type symptoms, who need more than exercise to get the ball rolling. EMS is also especially helpful in restoring muscle symmetry between right and left sides if a bulged or herniated disc causes especial weakness in one arm or leg.
Furthermore, writing more about electric stimulation is on the back burner as I build out the rest of SpineFITyoga for other reasons, including:
- Obtaining quality, fairly priced electric stimulation machines and electrodes/straps that work with them is currently a fiasco in the USA. A fiasco that I don't presently have time to deal with. It's not necessarily expensive, but it's a fiasco even if you have cash to burn.
- Electric stimulation, while effective and, for some, crucially important, for most isn't nearly as important for fitness, nor for decreasing neck and back pain, as learning what causes neck and back pain or SpineFITyoga's P5 and S5 programs.
- If you only do electric stimulation on your neck or back, you're only going to “feel better” in the short term and maybe even have stronger core muscles. However, you will probably continue to degenerate your spine at the same rate as before, leaving you with the same amount of pain in the long run.
- Electric stimulation with equipment good enough to help is considerably pricier than doing SpineFITyoga, with an ideal setup costing a few hundred dollars. If you pay thousands, you're really getting ripped off.
- Some of what I teach regarding electric stimulation is controversial. While I'm confident that I'm right and everyone else is wrong, if enough people use my methods, I help a million and hurt one, and even if coincidentally, someone's likely to make a big deal out of the one. So know this: I describe EMS as I do it, or did it. I'm not telling anyone else they should do the same. So copy at your own risk. I don't have a pacemaker, and I would not do EMS or TENS if I did without clearing it with my cardiologist first. Medical literature has reported dangerous and painful interference.
All that said, I'm a unique voice in the field of electric stimulation. I've been blogging on the subject for years, and I did a yearlong self-experiment where electric stimulation was my only form of exercise. As far as I know, I'm the only person to have ever done that. In doing so, I was able to directly apply what I was learning in the research to myself to see and feel what worked and what didn't, as well as advantages and disadvantages in comparison to conventional exercise. At the same time, I was able to apply what I was learning to most of my patients with their exercise programs in my physical therapy office. In doing so, I was able to give electric stimulation a shot for anything I thought it might help with, which was a lot of varying diagnoses.
Anyway, below are my favorite EMS electrode placements. I'm adding a “Chad's Rating,“ my subjective 0-10 scale, with zero being worthless and 10 being the best thing ever. If I rate something higher than an 8/10, I'll say that's better than conventional exercise for that isolated muscle group or body part only.

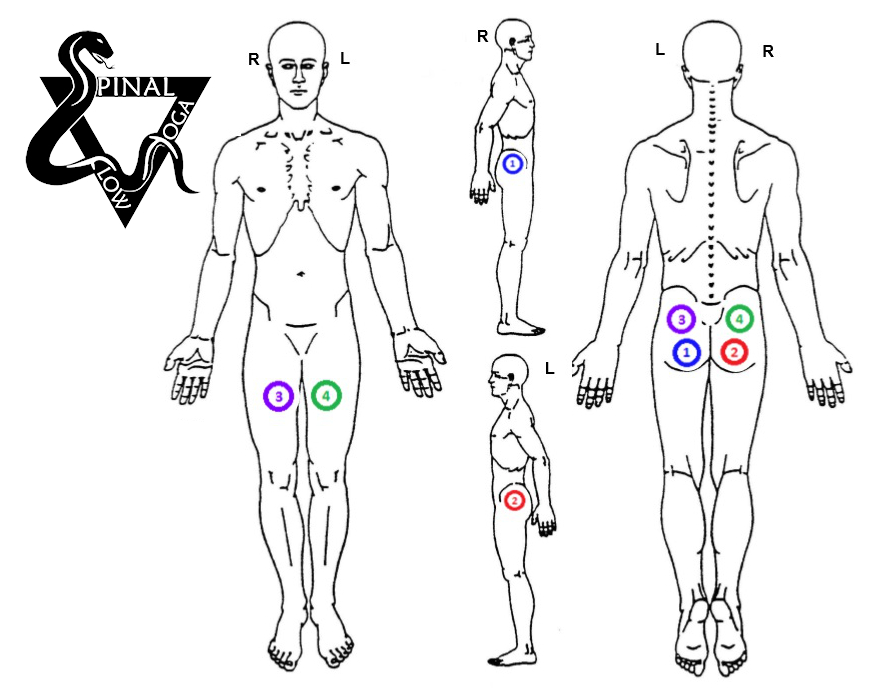
Core-1 (EMS for low back pain, abdominal/core strength)
Chad's Rating: 9/10
Brief Description
Core-1 is my favorite EMS pattern to get started, either for abdominal strengthening or immediately and substantially decreasing low back pain.
This pattern trains all abdominal muscles, stabilizing the low back, including the rectus abdominis (the six-pack), obliques, transverse abdominis, plus the spine extensors, all at the same time.
Because the EMS channels 1-4 are separated per region, you can go harder on the low back (channel 4), less so on the anterior abdominals (channels 1-2), and intermediate on the obliques (channel 3), which at first is what almost everyone prefers.
The first time I did Core-1, I thought, “If I turn this up any higher, I'm going to have a hernia right now! Anymore and it will tear my muscles!“
Fortunately, you get used to it. However, EMS is like exercise; if you don't go hard, it's not going to do much.

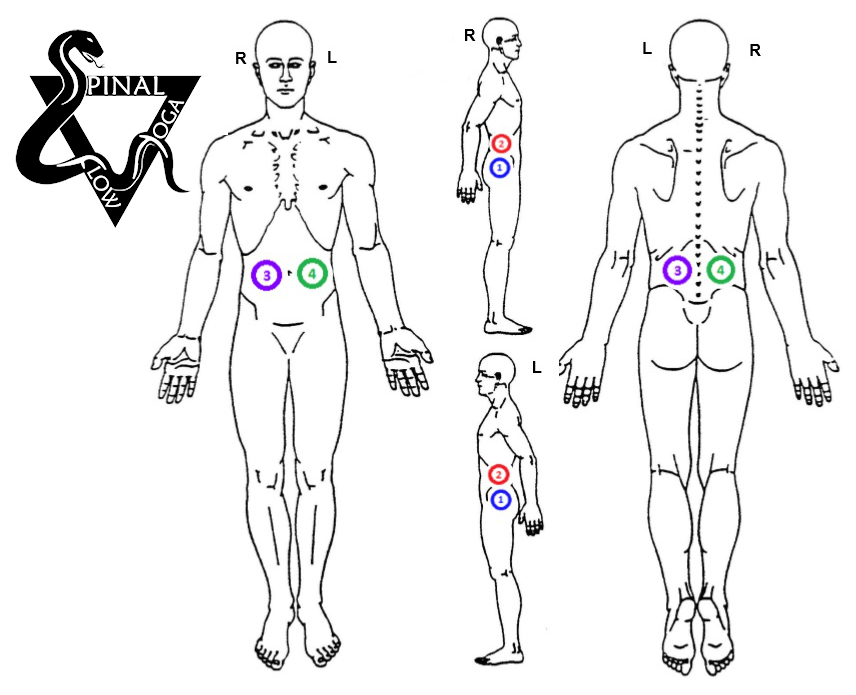
Core-2 (EMS for low back pain, abdominal/core strength)
Chad's Rating: 10/10
Brief Description
Core-2 is my favorite EMS pattern for advanced abdominal strengthening and decreasing low back pain. Like Core-1, this pattern trains all muscles stabilizing the low back at the same time.
The difference is the channels are crisscrossed, thus spaced further apart, allowing for deeper stimulation, stronger, and more unified muscle contractions.
However, because the electrodes of each channel are crisscrossed, you lose the ability to target specific muscle groups with greater or lesser intensity. Meaning you can't go harder on your low back, perhaps to further decrease pain, without overwhelming your anterior abdominal muscles.
After several weeks of training, the anterior abdominal muscles toughened up so that they can handle as much stimulation as your sides or back.
During the EMS blast with Core-2, it should feel like you are being crushed by an anaconda, almost literally.

Core-3 (EMS for low back pain, abdominal/core strength)
Chad's Rating: 7/10
Brief Description
Core-3 I rarely use, preferring to get the side abdominal (oblique) muscle contractions of Core-1 and Core-2.
With Core-3, you are trading off the oblique muscle stimulation to get an additional 2 electrodes on the spine extensors.
I'll do this if the person's low back pain is higher up than usual (upper lumbar/lower thoracic region). You want to make sure the electrodes are all below the ribs, keeping the stimulation away from the heart.
Another reason I might use this pattern would be post-pregnancy in women with diastasis recti, where I would want to strengthen her anterior abdominals and low back but not have her transverse abdominis and oblique muscles pulling so hard and potentially overstretching the already increased gap between both sides of her rectus abdominis muscle.
With Core-3, rather than being wrapped by a snake, it feels like you are being squished, front to back, in a vise.

TENS for Dysmenorrhea (Menstrual Cramps)
Chad's Rating: 6/10
Brief Description
I don't have a lot of experience with this one, obviously. However, I have read several papers on TENS for dysmenorrhea. It's not so much that I'm interested in women's health; I'm interested in all things EMS/TENS, and this came up in the research.
My office staff at the time was largely female, and they wanted to try it. The following pad placement is what they liked best, and they said it helped. Relief seemed to last only when the electric stimulation was applied, so I would think you would want a smaller 2-channel stimulator like the Twin Stim 4 that could be clipped on the belt and worn longer. Being on longer, I think you would want to do lower-intensity TENS rather than high-intensity EMS.
Notice that the electrode placement is about the same as the lower pads on all my core placements? It makes me think that if dysmenorrhea has a central sensitization component (from having hurt so long, over so many years), then Core EMS done regularly (every third day, I think, is ideal) and intensely might, over time, lessen pain from dysmenorrhea.
This is just a theory; however, it would jibe with what I have observed with chronic migraine sufferers. Whereas those who did my headache EMS program several times a week, even when they did not have migraines, steadily reported a lessening in both frequency and intensity of migraines, eventually to the point of being cured. Dysmenorrhea is not the same, I'm sure, but I suspect parallels. Thus, if anyone wants to report back with their experiences, I would love to hear it.
EMS for Neck Pain and Weakness
Chad's Rating: 10/10
Brief Description
Everyone will tell you not to stim the neck, particularly not the front of the neck, saying it is a “contraindication…“
…or at least they did. As of late, they are selling electric stimulation machines that only stim the front of the neck in what's now called vagus nerve stimulation.
However, despite what electric stimulation textbooks and the manual that comes with your stimulator say, electric stimulation to the neck is not a contraindication. It's merely a “precaution” that's been there since the 70s, and nobody has bothered to go on record to confirm or deny.
Since the 70s, I have been able to locate zero case reports of anyone being injured by doing so, despite a fair amount of research outside the field of physical therapy and fitness suggesting it is safe. I'm not saying it's safe, but I have been doing it to myself (aggressively) for years and also for years to my patients (much less aggressively).
In doing so, I got measurable neck muscle hypertrophy, and my neck muscle endurance tripled.
My patients reported subjective increases in neck strength, endurance, stability, and range of motion, corresponding with usual immediate and substantial pain reduction. Like them saying a 6/10 pain is being reduced to 1-2/10 on the very first try (with the right machine, right pads, right program, and right intensity). With them saying the pain reduction usually lasting at least a couple of days.
I'll add that while I have not used electric stimulation to treat dysphagia (difficulty swallowing) post-stroke, I'm familiar with parameters used by the VitalStim unit, promoted to speech therapists for that purpose. My thoughts are that the VitalStim manufacturers don't know the first thing about electric stimulation for improving muscle performance, including the swallowing muscles, and it shows in the dismal results in independent research of their device. Still, I think the concept has merit, and
I'll add that it's my recollection that the Twin Stim 4 has more than twice the power and infinitely more versatility regarding programming at roughly 1/20th the cost. Yes, one-twentieth; as I said, electric stimulation in the USA is a fiasco.

Full-Spine TENS for Pain
Chad's Rating: 7/10
Brief Description
This placement being unbalanced is not ideal for EMS. However, for TENS (turned up, with large electrodes), it often results in remarkable pain reduction, particularly in those affected with chronic, widespread, central sensitized, fibromyalgia-like pain. Those patients for whom even the lowest intensity exercise with good posture exacerbates pain, making them afraid to try any exercise.
My FM-TENS program with this placement feels pretty amazing even if you don't have pain.
It's unfortunately difficult to self-apply the electrodes, but with straps and lying flat on one's back, sans pillows.
For those with pain “everywhere” that prevents even good exercise from helping. FM-TENS to the entire spine, gradually adding EMS to the hips, legs, and core, is generally very well tolerated.
Intermittent fasting helps too and starts decreasing weight and systemic inflammation without requiring any physical exertion. Gradually adding P5 to learn good posture and coordination with minimal exertion and finally progressing to S5 to at last build strength and endurance is what I would do if it were me in a worst-case scenario (anxiety, depression, overweight, widespread pain seemingly everywhere). I'll have more to say on this later.
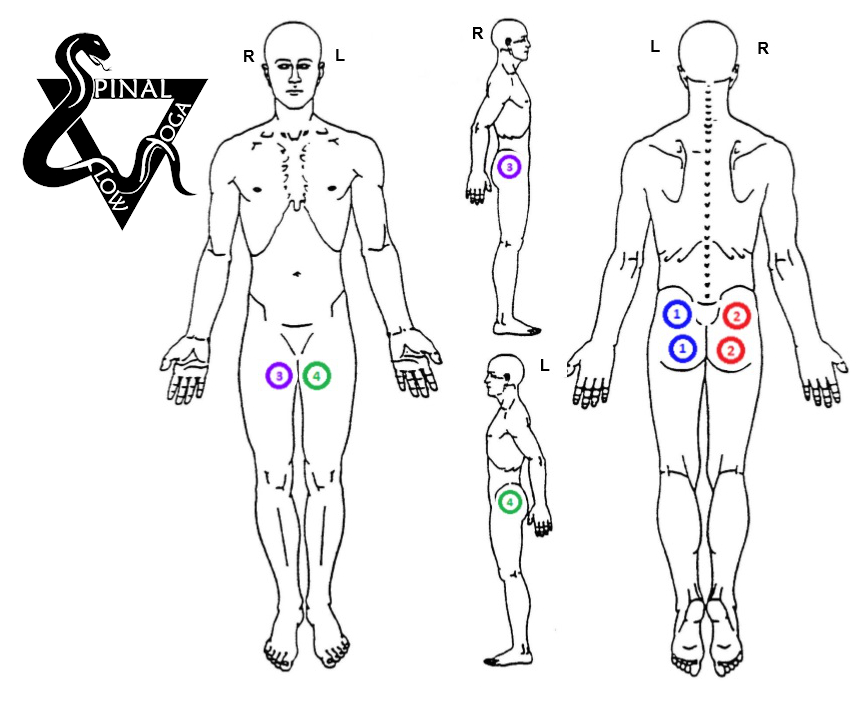
Hips-1 (EMS for increasing global hip strength)
Chad's Rating: 7/10
Brief Description
Hips-1 was a surprisingly effective stimulation pattern I discovered in my year of EMS. Compression shorts help hold the electrodes in place, but I'd put my elastic straps over the shorts, keeping the electrodes as tight to the skin as possible.
I use only rubber carbon electrodes, for which you want to always keep them tight and very wet with tap water, because if contact is poor, they'll sting. The inner thigh electrodes from channels 3 and 4 are to be placed inside the thigh, as high up as possible, NOT facing the front as shown in the image.
An update here would be that strapping all four electrodes into place and getting them to stay put without the wires pulling loose is tedious. As such, even with a four-channel stimulator like the Globus, I've come to only use the first two channels and not worry about the inner or outer thigh. This makes a simulator like the less expensive Twin Stim 4 very viable.
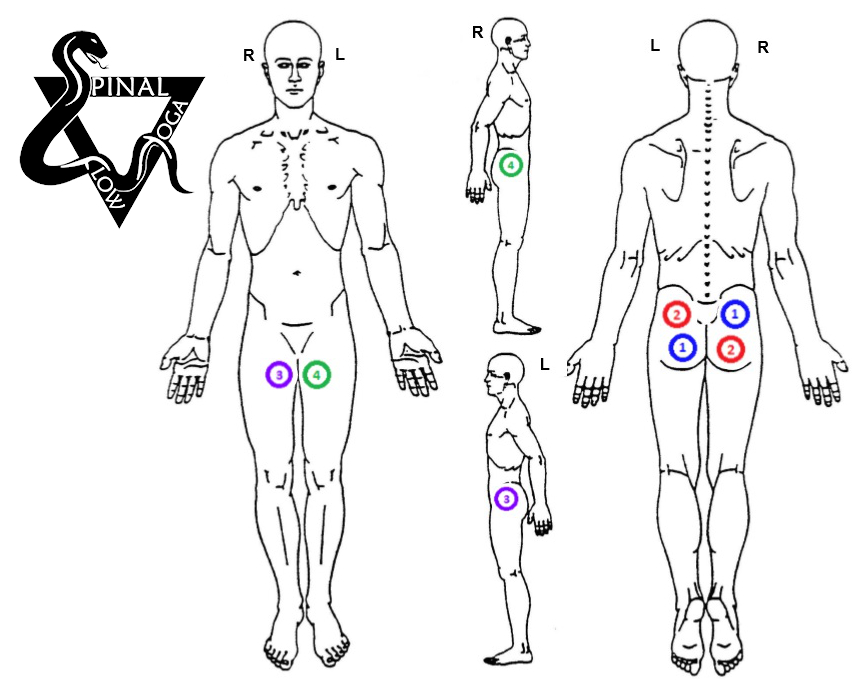
Hips-2 (EMS for increasing global hip strength)
Chad's Rating: 8/10
Brief Description
Hips-2 is the same as Hips-1, but there is more crisscrossing of the electrodes, getting each channel further from each other for deeper stimulation. Hips-2 does feel better to me, but like Core-2, it's better after you have been doing EMS for a while and all your muscles are conditioned to tolerate the same intensity of EMS. Otherwise, some muscles will either feel overworked or underworked. And yes, EMS hits hard enough that it can strain/injure muscles, tendons, and ligaments if you overdo it. That said, overdoing it causes a LOT of sensation, so it is very unlikely to happen accidentally, and all EMS machines I like ramp up slowly and steadily, making overstimulation unlikely.
Update like above: strapping all four electrodes into place and getting them to stay put without the wires pulling loose as you get comfortable is tedious. As such, even with a four-channel stimulator like the Globus, I've come to only use the first two channels and not worry about inner or outer thigh. This makes a simulator like the TS4 very viable.
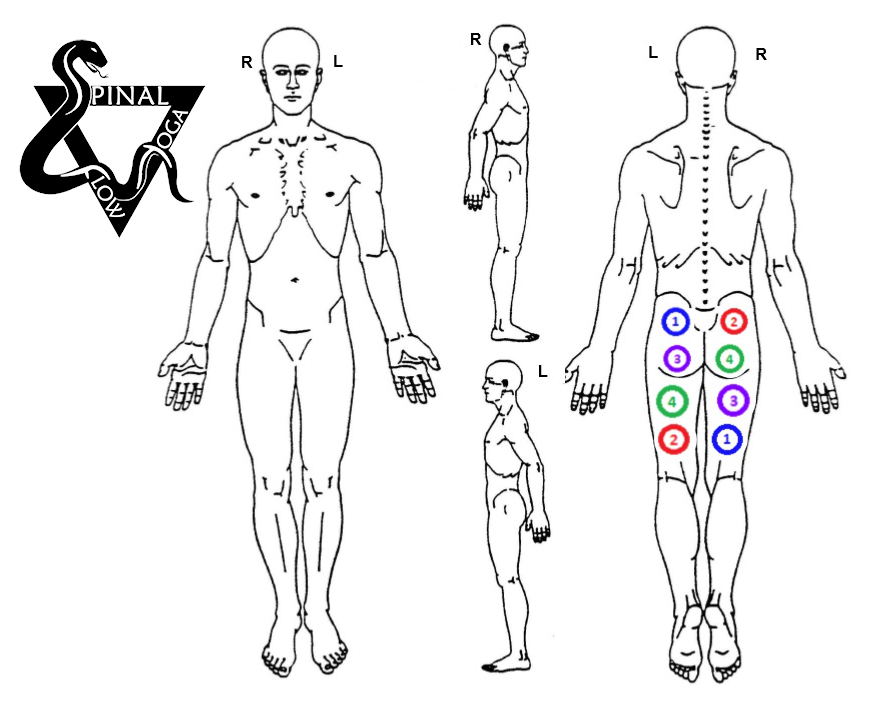
Hips-3 (EMS for increasing global hip strength)
Chad's Rating: 9/10
Brief Description
Hips-3 is the same concept (crisscrossing electrodes) as Hips-2 but taken even further for maximal depth of muscle contractions. The difference is noticeable, making this my new go-to pad placement for hip musculature, leading to changes in feel during stimulation, next-day muscle soreness, and fatigue. That said, if you can work up to the Level-3 Lunges of F5, you'll probably not feel any hip or leg EMS is necessary.
Still, I think this can be an adjunct if you have gluteal muscle damage, which I believe results from too long of sitting. This is what I think Stuart McGill is referring to when he talks of "gluteal amnesia," however I think it's more of a pressure-induced muscle fiber injury or nerve palsy.
This might show up when performing the lunges of S5 as both a low number of reps and knee pain. Which I think results from a relative overuse of quadriceps (front thigh muscles) having to extend the knee, compensating for the glutes not pulling their weight (literally) to extend the hips. Thus, the glutes are insufficiently assisting in what should be a compound knee and hip exercise.
If combining hip EMS with lunges, I would definitely do them after lunging but on the same day. This is to minimize glute fatigue during lunges (which would only worsen quadriceps over-utilization in the near term) and to allow for the longest recovery time before lunging again 3 days later.

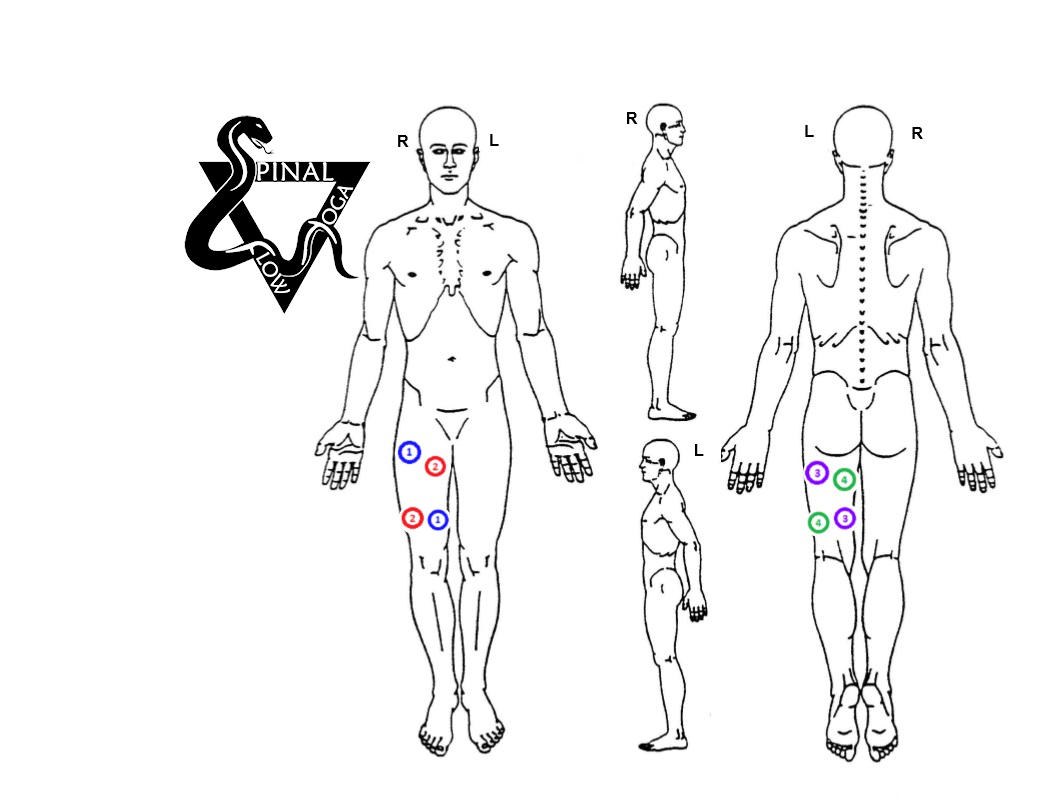
Hip-Thigh EMS
Chad's Rating: 4/10
Brief Description
Hip-Thigh is placement I rarely use. Hips 1-3 work better for hips, and Basic Thigh works better for quadriceps and hamstrings.
However, Hip-Thigh is worth using for someone who has recently had a large and painful lumbar disc herniation causing pain and weakness in one of the legs.
Furthermore, EMS to the weaker side is a good way to prevent pain from becoming weakness on the affected side. After the disc inflammation calms down and the body starts to reabsorb the fragment, leg pain should diminish so that active exercise (P5 and F5) can be initiated.
Ideally, in such situations, the person would be doing Core EMS 1-3 concurrently.
Unfortunately, EMS and TENS don't work as well for pain during an acute disc blowout as they do when people have chronic/recurrent pain. However, it usually helps some with pain while increasing muscle strength. I don't expect "miracles" with acute pain (less than 8 or so weeks) quite the same as I do with chronic pain, where people are often like, "Wow!"
The good news with acute pain is it's more likely to improve on its own, so long as you stop doing what's causing it.
EMS for Trochanteric “Bursitis”
Chad's Rating: 3/10
Brief Description
Trochanteric "bursitis” is seldom bursitis but is gluteal or trochanteric tendinopathy, hopefully not progressing to muscle tearing.
That said, bursitis is what everyone thinks it is, and in my experience, EMS helps restore strength to the affected muscle and helps reduce pain at the same time.
If you have your own machine, running one of the Core 1-3 programs, followed by one of the Hip 1-3 programs, is better. But if you are in physical therapy and have time to run only one program, this pad placement is a fair compromise.
The real exercise of F5 is almost certainly better also, but if you have the means, EMS afterward should accelerate progress. If you have the greater surface area of the giant 5×8" rubber carbon electrodes, this placement is fairly fantastic all by itself, which is how I did it in my office.
The lower 3/10 rating reflects that S5 still works better and only takes 5 minutes to finish.

Glute-Hamstring-1: EMS for glute and hamstring circulation and hypertrophy
Chad's Rating: 6/10
Brief Description
This is probably one of the better electrode placements to prevent and/or recover from pressure ulcers for someone in a wheelchair (likely to work only if they have spasticity).
Unfortunately, this only works if the connection between the muscle and the lower spine is still intact (because of an injury higher in the spine). Meaning it should help someone with quadriplegia but not paraplegia.
If it works, this placement should both improve circulation in the skin and muscles and increase muscle mass, thus taking pressure off the sit bones. In such a situation, I would very likely want to use one of my combination programs where I combine the strengthening of a 10-50-10 program with a 5 Hz aerobic EMS program turned up during the rest period between EMS blasts. Otherwise, you would have to run two separate programs to get both effects, which isn't the worst thing in the world.
Glute-Hamstring-2: EMS for glute and hamstring circulation and hypertrophy
Chad's Rating: 6/10
Brief Description
Same intention and purpose as the above; however, the electrodes are crisscrossed, getting each end of a channel further from its sibling. The increased distance increases the depth of muscle contraction. Generally this is desirable, but like my other crisscross placements, you lose the ability to localize exactly where you want a weaker or stronger muscle contraction.
Basic Thigh: EMS for Quadriceps and Hamstring Strength
Chad's Rating: 7/10
Brief Description
This is my absolute go-to thigh placement. If I'm rehabilitating a knee after almost any surgery. Or if one leg has arthritis or some injury that does not let me train it as hard (or at all) with regular exercise, I'll very likely use Basic Thigh.
Placing 2 sticky electrodes on the quadriceps for some “mild tingling” is a joke when instead I can strap 4 large crisscrossed rubber carbon electrodes on the same quad, and while I'm at it, put another 4 crisscrossed electrodes on the hamstrings.
The balancing of quadriceps and hamstrings gives you AT LEAST double the overall strength and endurance.
Wherefore the co-contraction of the EMS balances forces, lessening shear stress about the knee while you are at it.
Knee pain should be reduced more also, per my experience in the physical therapy office and per gate control theory.

Aerobic EMS or TENS
Chad's Rating: 7/10
Brief Description
This electrode placement is what I used experimenting with aerobic conditioning with EMS.
To make it work best, I needed giant 5"x8" electrodes. The extra-wide electrodes very much dispersed the current density (how much electricity is going through each square inch of electrode, allowing me to tolerate overall higher levels of stim), and sibling electrodes being on alternate legs allowed for very deep stimulation.
My heart rate did hit aerobic levels. I was both breathing hard and sweating. It was not comfortable, and I would have preferred real exercise. However, for someone who otherwise can't exercise, and for those whose diminished sensation lessens pain, this could be the best option.
Furthermore, when I was testing it for my blog, I was going as hard as I could to get my heart rate up; less intensity, just getting the muscles twitching, still improves circulation.

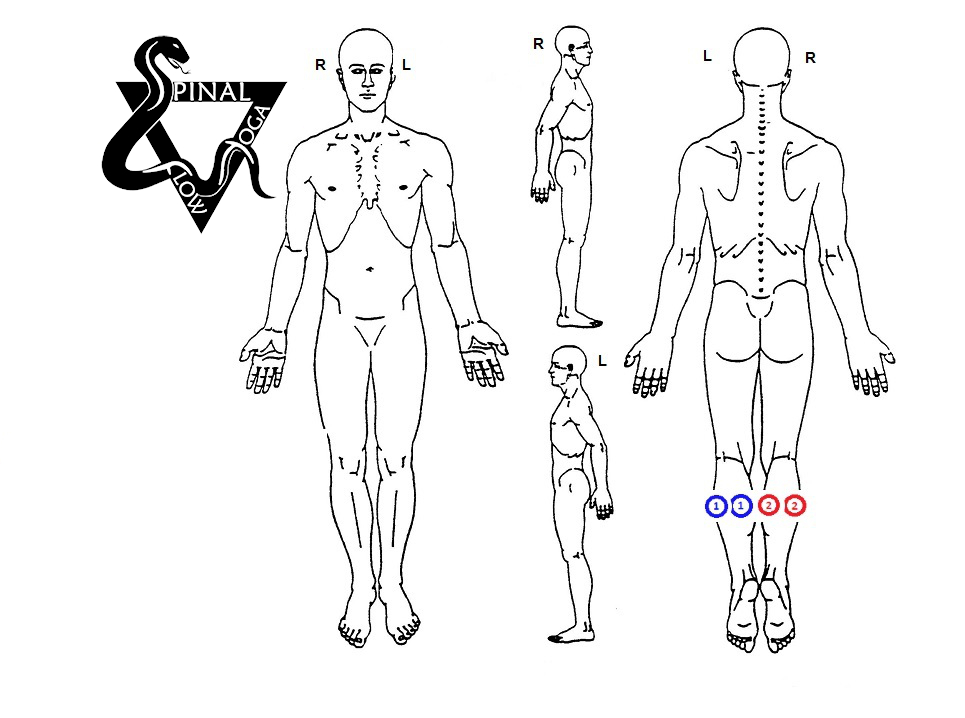
Anti-Blood Clot, Deep Vein Thrombosis EMS
Chad's Rating: 6/10
Brief Description
This pattern is what I have used for post-total-hip and other surgeries to lessen the risk of deep vein thrombosis (DVTs, aka blood clots), based on this blog/research.
What's cool is that a good EMS machine can easily be programmed to strengthen muscles as well as improve circulation.
Both legs are being stimulated because research has shown blood clots sometimes form in the non-operative leg due to post-surgical inactivity. I would suggest asking your surgeon about this, perhaps being able to hand him the paper cited in my blog.
I would rate this higher; however, I now think my basic foot stim pattern works at least as well, is easier to apply, and only requires one channel. So the Twin Stim 4 would work just as well for a lot less money.

Neuropathy or Plantar Fasciitis EMS
Chad's Rating: 8/10
(I would rate this one higher if not for it being supplanted by the much simpler basic foot below, and the purple/green placements (channels 3 and 4) are of less importance than blue and red (channels 1 and 2). So if you have only a good two-channel stimulator like the TwinStim 4, you're golden.
Brief Description
EMS for neuropathy works considerably better than expected.
With patients of mine reporting 8 or 10/10 pain decreasing to 0/10 pain, frequently, if not usually, after their first EMS treatment with my 10-50-10.
Since I'm not treating people in the office anymore, I'm unable to test my latest ideas on neuropathy. I'm all but positive that the combination of the above-mentioned EMS program with 5 Hz aerobic EMS programmed into the rest period would work even better.
I used to stand on the electrodes and have my patients do the same based on what sprint coach Charlie Francis said he did to prevent foot cramping. However, now I don't think foot cramping is a problem, so now I strap electrodes to the bottom of my feet if I want to do it, sit back, and read a book, rather than standing there for ten minutes.
If you have neuropathy, probably you should do F5, at least level 1. And maybe you should think about intermittent fasting, but I'll bet a million dollars that EMS works a lot better, a lot faster. It's one of the few instances where EMS is far ahead of exercise, even SpineFITyoga.
See the Basic Foot placement below, because it's far simpler, easier to apply, and, I expect, even better.

Basic Foot EMS
Chad's Rating: 10/10
Brief Description
One of my current favorites!
This simple placement has become my go-to pattern for intrinsic foot muscles. If the EMS machine is powerful enough and the nerves healthy enough, you can feel and strengthen everything up to your knees.
The electrodes being so far apart (the length of both legs) causes the current to run VERY deep. Thus, when trying to rehab my own foot injury, I used this pattern with the 10-50-10 program, and it felt very strong, but not unbearable in sitting. However, it certainly took some getting used to.
Because of simplicity and speed of application, this would be the first placement I would try for neuropathy or plantar fasciitis, also posterior tibial tendinopathy, or any time I wanted to strengthen the muscles within the foot and even calf musculature.
Calf EMS
Chad's Rating: 3/10
Brief Description
This is very strong EMS, and arguably too strong. Such that I required something fixed (like a leg press machine or the other side of a hallway) to brace the ankle against during the blast to prevent extraordinary cramping.
The need to brace the ankle makes real exercises, calf raises, either in the gym or as I teach them in SpineFITyoga's F5, preferable.
However, if there is nerve damage, either in the leg or in the spine from a herniated disc, EMS to the affected side, combined with real exercise, should be state of the art.
Merely standing with body weight on both or even one foot is not enough if your calves get strong but is often good enough when still weakened.

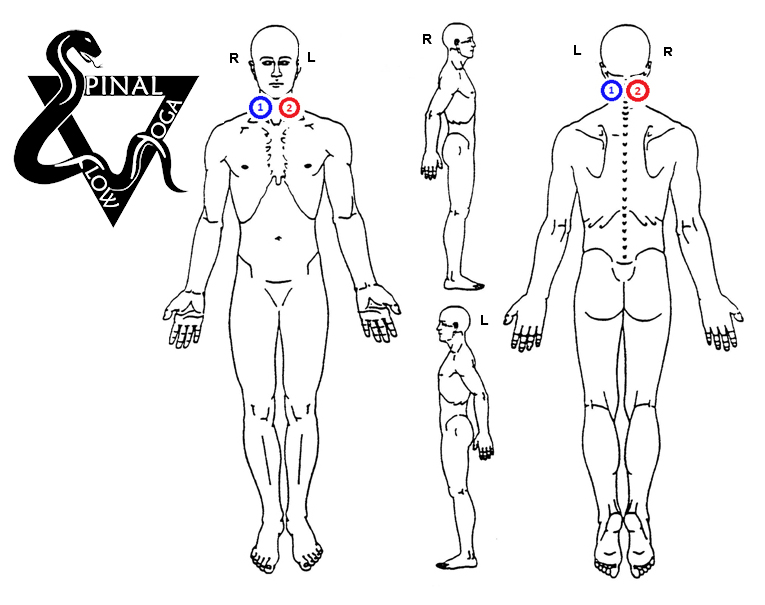
Headache EMS
Chad's Rating: 10/10
Brief Description
I think it would be most logical to present my EMS patterns top-down, from head to feet. However, I would rather not start out with my most controversial placements, even if it is one of the best.
Notice these electrodes are NOT crisscrossed and ARE right next to each other, almost touching, as I DON'T want deep stimulation. I want to keep the stimulation superficial, which, in my experience, works extremely well for both tension headaches and occasional migraines, and even chronic migraines.
Definitely read everything I have written regarding headaches and electric stimulation and see that this is evidence-based. Fortunately, the head is sensitive so that people don't need to go as high for benefit and can't go as high because high-intensity stim on the forehead is intolerable.
EMS for headaches and neuropathic pain are the closest things to miracle cures I am aware of. That's using my programs and large rubber carbon electrodes, which I think is why my results are so much more dramatic than in the research.

Basic Shoulder: Electric Stimulation
Chad's Rating: 3/10
Brief Description
I don't love EMS to the shoulder, or any arm muscles, actually. But I'll list a few placements because sometimes they are necessary and helpful. The difficulties in strapping the electrodes in place, especially on yourself, make conventional exercise generally preferable. This pad placement is simple enough, targets most of the rotator cuff as well as the upper arm, and can decrease pain while helping to restore lost muscle strength.
In the clinic, we would often use TENS programs like this to lessen pain, but with light enough intensity to avoid muscle contractions early post shoulder surgery.

Frozen Shoulder: Electric Stimulation
Chad's Rating: 4/10
Brief Description
Similar to the above but with an extra channel, thus hitting the rotator cuff and deltoid harder. While for most shoulder conditions I think EMS is of only moderate utility, for frozen shoulder (aka adhesive capsulitis) I've had both EMS and TENS work very well, decreasing pain well enough that my patients could avoid both NSAIDs and cortisone injections, and better tolerate the stretching necessary to restore normal range of motion. For frozen shoulder, I have used both my FMTENS to decrease pain quickly, progressing 10-50-10 or 5-15-10 EMS programs to increase shoulder strength while still decreasing pain.

Whole Arm EMS
Chad's Rating: 3/10
Brief Description
This is a stim pattern that I would likely do for rehab after an injury to one side or if there were nerve damage causing weakness to that side.
Though I did it on myself for a year as part of my experiment, and it worked, in my experience, lifting weights or doing S5 is better.
"Hand grip stimulator" means hand grip "electrode," which is a specialized electrode for delivering the electric stimulation to the palm of the hand. I have had this work very well in people with neuropathy of the hands, sometimes seen in diabetics.
I've used this for tennis elbow, golfer's elbow, aka shooter's elbow, in the population I saw most, but I would say the exercise alone is responsible for 90% of the recovery.

Electric Stimulation for De Quervain Syndrome
Chad's Rating: 3/10
Brief Description
This electrode placement has worked well with my patients after strengthening exercise of the arm and wrist muscles, very similar to the protocol used in my shooter's elbow treatment. Followed by what's at first a painful stretch, mimicking the Finkelstein's test.
I would do the 10-50-10 program as tolerated, and I have had patients, within 2-4 weeks, be pain-free and their bad arm stronger than their good arm. As above, the “hand grip stimulator“ denotes a hand grip electrode.
SpineFITyoga

First self-paced NEUTRAL-SPINE YOGA for Spine Health AND Total Body Fitness
- Fast: 5-minute per day, home programs.
- Expert: Designed by a Physical Therapist with 20 years clinical experience.
- Guaranteed: Results in 40 Days or Your Money Back.
